Immunotherapy is an increasingly important strategy for fighting cancer. The body’s own immune system is encouraged to attack tumours, via cancer antigens on the surface of the cancer cells that distinguish them from healthy cells. There are several ways in which this can be done. The most widespread in clinical practice is the use of monoclonal antibodies that bind to the cancer antibodies; many familiar products fall into this category, such as trastuzumab (Herceptin), alemtuzumab (Campath), rituximab (Rituxan/MabThera) and bevacizumab (Avastin). Cytokines, notably the interferons and the interleukins, can also be used to alter a tumour’s immune response.
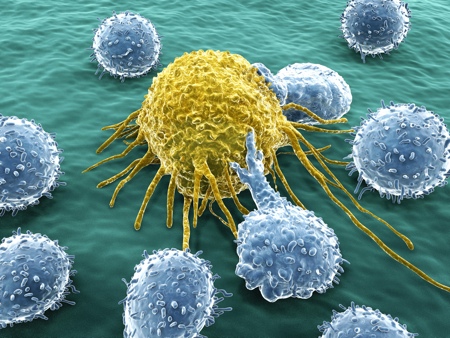
There is a third alternative – cell-based therapies. Dendritic cells were discovered in the early 1970s by Canadian scientist Ralph Steinman at Rockefeller University in New York, a discovery that won him a share in the 2011 Nobel prize in physiology or medicine.1 They essentially act as a switch that turns the immune system on and off. They pick up foreign antigens from invading cells, and then activate the T-cell lymphocytes with these antigens so they are primed to destroy the alien cancer cells bearing these antigens.






