The molecule camptothecin was isolated from the bark of the Chinese Camptotheca acuminata tree, which is used in traditional Chinese medicine. Camptothecin is used as an anticancer agent, as it inhibits topoisomerase I, an enzyme that is involved in the cell reproduction cycle.
The drug stabilises the transient covalent linkage that the enzyme forms with the DNA strand, causing the DNA to break; this mechanism of action is not seen in other classes of anticancer agents. However, it failed in clinical trials because it caused severe side-effects and its pharmacology proved unpredictable.
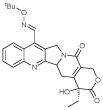
Numerous semisynthetic analogues have been developed in the hope of finding a more acceptable drug with the same activity. Topotecan and irinotecan are already on the market, and another, the orally available gimatecan, was discovered by Sigma-Tau and has been licensed to Novartis for development.1
A dose escalating Phase I/II trial was carried out in 12 adult patients with recurrent malignant gliomas.2 Subjects were given 0.33 to 1.1 mg/m2 of the drug orally for five days every 28 days. It was well tolerated, and no dose limiting toxicity was observed. After two cycles, four of the seven patients who were not also receiving antiepileptic drugs had a radiographic response of disease stabilisation. However, none of the five who were on antiepileptics had a response.
A total of 108 patients with advanced solid tumours took part in another dose escalating Phase I trial.3 They were given oral doses of 0.8 to 7.2mg/m2 per cycle once a day for five days a week for one, two or three weeks every 28 days. Its tolerability depended on the schedule, and the main side effects that were observed included myelosuppression and thrombocytopoenia. Some nausea and vomiting were seen, and it was highest on the one-week schedule. Six patients experienced a partial response. The drug's long half life meant some accumulation in the plasma was seen.
Phase II trials are also being carried out. In one, 43 patients with advanced breast cancer that had previously been treated with anthracycline and a taxane were given oral doses of 4 to 5mg/m2 per cycle for five days a week on weeks 1 and 2 every 4 weeks, with the dose being reduced from 4 to 5mg/m2 because of high levels of thrombocytopoenia developing.4 Of the 18 initially evaluable patients, three had confirmed partial responses lasting up to nine months, and there were two unconfirmed partial responses.
Another multicentre Phase II trial looked at the drug in 40 patients with advanced or metastatic soft tissue sarcoma which had relapsed after anthracycline/ifosfamide based regimens.5 They were given 0.8 mg/m2 a day orally for five days every 28 days, and the best overall response was stable disease in 37.5% of subjects. Ten of these had stable disease for at least four months. However, enrolment was halted because of lack of efficiency. Trials continue for advanced solid tumours, gliomas and myelodysplastic syndrome.






