A number of anticancer agents are targeted at the epidermal growth factor receptor signalling cascade – EGFR, or erbB-1 – and drugs such as trastuzumab (Herceptin) have activity against erbB-2, also known as HER-2.
All the proteins in the erbB family are trans-membrane receptors, with an extracellular ligand binding domain and a tyrosine kinase domain within the cell, linked across the cell membrane. Ligand binding causes a conformational change, setting off signal cascades within the cell that lead to production of downstream mediators. This gives rise to the expression of genes with cellular functions such as the inhibition of apoptosis and increasing proliferation.
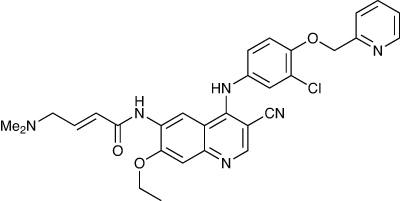
But the development of resistance to anti-erbB drugs is a problem, and so a second generation of drugs is being developed. These form covalent bonds with the receptor, permanently blocking it. Neratinib is one such compound. It works across different erbB receptors, and is being developed by Pfizer.1
In a Phase I dose escalation trial in patients with advanced solid tumours, the drug was given orally as a single dose, followed by a one-week observation period, and then once a day continuously.2 The aim was to escalate the doses from 40 to 500mg. One patient given 180mg and four given 400mg experienced a dose-limiting toxicity of grade 3 diarrhoea, so the maximum tolerated dose was set at 320mg, with the pharmacokinetics supporting a once-daily dosing regimen. Other toxicities included nausea, vomiting, anorexia and fatigue.
Eight of the 25 evaluable breast cancer patients saw a partial response and one stable disease for more than 24 weeks, and six of the 14 evaluable NSCLC patients also achieved stable disease.
An open label Phase II trial has also been carried out.3 A total of 136 patients with advanced erbB-2-positive breast cancer, 66 of whom had previously been treated with trastuzumab, were given 240mg of the drug orally once a day. The 16-week progression-free survival rates were 59% for the 63 evaluable pre-treated patients, and 78% for the 64 evaluable patients in the naïve group. The median progression-free survival was 22.3 and 39.6 weeks respectively, and the objective response rates 24% and 56%. Similar side-effect profiles were seen to those in the Phase I trial, and while some patients had their doses reduced, only one discontinued treatment.
In a second Phase II trial, 167 patients with advanced NSCLC were profiled.4 Those who had at least 12 weeks of pre-treatment with a tyrosine kinase inhibitor were put into either arm A or arm B, depending on whether they were EFGR mutation positive or not. Arm C included naïve patients with adenocarcinoma and light smoking histories. They were given daily oral doses, initially 320mg but reduced to 240mg because of diarrhoea. The response rate was a disappointing 3% in the 91 patients in arm A, and zero in the other two. However, three patients with one specific mutation had a partial response, and a fourth achieved stable disease lasting 40 weeks. The low response might be a result of insufficient bioavailability because of the diarrhoea-limited doses.
references
1. R.H. Tsou et al. J. Med. Chem. 2005, 48, 1107
2. K.K. Wong et al. Clin. Cancer Res. 2009, 15, 2252
3. H.J. Burstein et al. J. Clin. Oncol. 2010, 28, 1301
4.L.V. Sequist et al. J. Clin. Oncol. 2010, 28, 3076






