Prostate cancer is the second most common cancer in men and is usually treated with hormone-based...
Prostate cancer is the second most common cancer affecting men, and it is usually treated with hormone-based therapies. However, over time, the cancer frequently becomes refractory to these drugs, leading to progression and metastasis. Docetaxel can be used once hormone treatments no longer work, but it has significant side-effects and its success is limited.
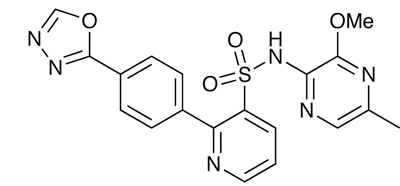
Another potential treatment strategy is to target endothelin-1, a signalling peptide that has a variety of physiological functions, and it appears that one of its receptors, ETB, is downregulated in prostate cancer cells, while ETA is overexpressed. Activation of this ETA receptor is thought to be involved in the progression of prostate cancer, including angiogenesis promotion and apoptosis inhibition. ETB may have the opposite effect. ETA thus has potential as a drug target. One such selective antagonist, zibotentan from AstraZeneca, is now in Phase III trials.1
Its potential was studied in a Phase I trial in patients with metastatic, hormone-resistant prostate cancer.2 Subjects were given escalating doses of oral zibotentan, from 10 to 200mg, once a day for 28 days. Those who showed a clinical benefit could receive further doses until they no longer benefited. The maximum tolerated dose was 15mg/day. No unexpected adverse events were observed, and a number of patients achieved prolonged stable disease.
In a randomised, doubleblind, placebo-controlled, parallel group Phase II trial, 312 patients whose hormone refractory prostate cancer had metastasised into the bones and were relatively pain free were given 10mg of zibotentan a day or placebo.3 While no statistically significant effect on time to progression was seen, there were indicators of overall survival increasing in the zibotentan group. Phase III trials are now under way, studying its efficacy alone, in combination with docetaxel and as an add-on to existing care.
References
1. R.H. Bradbury et al. J. Med. Chem. 1997, 40, 996
2. W.R. Schelman et al. Invest. New Drugs, pub online Sep 2009