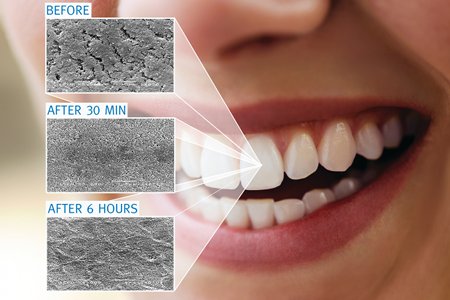
At this year's CPhI Pharma Awards BioClin won the Bronze Award for Best Innovation. This article takes an in-depth look at this innovative company and its prize-winning product Multi-Oral RemiDent.
The majority of infectious diseases are initiated by adhesion of pathogenic organisms to the tissues of the host. Pathogens usually colonise host tissues that are in contact with the external environment, typically the epithelial tissues – skin and mucosa.
The 2QR-complex, discovered and patented by BioClin together with the VU University in Amsterdam in 1998, consists of large negatively charged multi-branched polymers and has the unique ability to neutralise harmful microbes by blocking their adhesion to skin or mucosa. This effect is achieved by the capacity of the 2QR-polysaccharides to bind with the adhesion system on the cell surface of pathogenic micro-organisms. By blocking the ability of undesirable bacteria to bind and settle on the substrate and feed and multiply, beneficial bacteria are allowed to flourish, thereby inducing a process of competitive exclusion.
With the ‘neutralisation’ of pathogenic bacteria, 2QR-complex (pronounced to-cure) rebalances the microbial communities in and on humans. It can be used to treat and prevent a wide range of problems related to bacterial overgrowth, without causing any undesired adverse effects and can be applied in a wide variety of self-care and OTC products.
BioClin is a Dutch company, founded in 1989 by Dr Annelize Goedbloed and Floris Koumans. The company is part of the Orange Pearl Innovation Group, one of the leading innovation groups of the Netherlands. 2QR-complex is the name the inventors have given to this unique complex of polysaccharides that is derived from plants through a process of molecular ultra filtration (INCI name: Galactoarabinan Poly-glucoronic Acid Crosspolymer). This forms the basis of all BioClin’s medical devices (Class I and IIa) and personal care products.
2QR-complex is specific against a great number of (opportunistic) invasive pathogenic microbes
It is specific against a great number of (opportunistic) invasive pathogenic microbes by blocking their adhesion mechanism to the host tissue. This mode of action is selective and does not affect the desirable or commensal flora such as Lactobacilli.1
With this mode of action, the 2QR polysaccharides adhere to the cell membrane but do not penetrate the pathogens. Oral products – e.g. mouthwashes – are often based on disinfectant ingredients such as chlorhexidine. Such biocidal substances kill microbes by dissolving the cell wall. They are non-specific in this action and also kill useful bacteria thereby destroying the microbiota. Most of these disinfectants are toxic for tissue cells and impair healing. The 2QR-complex is not based on harsh or toxic substances; it does not affect the good and useful bacteria; it has no negative impact on the body’s own cells and their healing process; it does not provoke resistance and there are no negative side-effects.
One of the problematic areas for which BioClin has developed a product range based on the 2QR-complex is the oral cavity. A disrupted balance of the oral flora is directly connected with a range of interconnected oral problems, and the vicious circle of problems can be broken only by correcting the disturbed oral flora.
Medication is often the cause of dry mouth problems or other bacterial disturbances. Such problems are directly related to the demineralisation of the tooth enamel and the forming of plaque, which is also a main cause of gingivitis. Such problems can be treated with Multi-Oral RemiDent (previously named Remin) and it is also effective against tooth erosion, affected enamel or sensitive teeth.
The oral cavity differs from all other human microbial habitats by the simultaneous presence of two types of surfaces for microbial colonisation: shedding (mucosa); and the only known anatomical aspect of the human body that does not have a regulated system of shedding surfaces – the teeth. This allows numerous micro-organisms to adhere to the surface of the teeth over time.
These multiple species of bacteria become a biofilm (dental plaque), which is composed of about a thousand bacteria that take part in the complex ecosystems of the mouth. Dental plaque can give rise to dental caries (tooth decay) and periodontal problems such as gingivitis and chronic periodontitis.
Among the oral diseases, dental caries is the most common chronic disease of mankind.2 It is a complex and dynamic process in which a multitude of factors influence and initiate the progression of disease. It is profoundly affected by factors such as oral hygiene and saliva.3
Tooth enamel is the hardest mineralised skeletal tissue present in the body. Its primary mineral is hydroxylapatite, which is a crystalline calcium phosphate. Enamel is a-vascular and has no nerve supply within it. This means that it can be irreversibly lost. However, it can undergo mineralisation changes.
Enamel can be strengthened by a process called remineralisation: adding minerals to the enamel matrix through the saliva. Enamel is weakened by demineralisation, which is the stripping of minerals from the enamel. The enamel is in a state of constant flux between the two states. When the acids begin to dissolve the mineral more quickly than the saliva can replace, a cavity is created.
Remineralisation is the natural repair process for non-cavitated lesions, and relies on calcium and phosphate ions to rebuild a new surface on existing crystal remnants in subsurface lesions remaining after demineralisation.
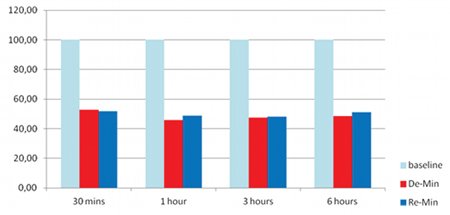
Figure 1: Control group with artificial saliva: results of the control group with regular human saliva showing slight remineralisation
Saliva is one of the most important factors that influences the development of dental caries.4 The saliva circulating in the mouth at any given time is termed as whole saliva and consists of a mixture of secretions from the major and minor salivary glands and traces from the gingival crevicular fluid. By constantly bathing the teeth and oral mucosa, the saliva functions as a cleansing solution, a lubricant, a buffer and an ion reservoir of calcium and phosphate, which are essential for remineralisation of initial carious lesions. Saliva promotes oral health and hence lack of its secretion contributes to the disease process.3, 5
To combat the common problem of demineralisation, BioClin developed Multi-Oral RemiDent, a remineralisation gel for application in the oral cavity with a specially developed patented applicator. The product is intended to treat and prevent bleeding gums and tooth erosion, reinforce tooth enamel, prevent plaque formation and condition the gums, neutralise harmful bacteria and optimise the oral flora.
Besides the 2QR-complex that eliminates the discomforts of irritated tissue, Multi-Oral RemiDent contains a remineralisation agent, an antioxidant agent, bioadhesive thickeners and ingredients with strong antiplaque properties as active ingredients. It forms an invisible bioactive barrier over the gums and teeth, creating a barrier against pathogenic microbes.
The product is packed in an aluminum tube of 50ml with applicator. By applying it with the flexible tip of the applicator, the gel is pushed into the pockets in between the teeth and into the gap between the gums and the teeth, where the product should be most active. It should be used after brushing the teeth last thing at night, so that the gel has a long contact with the tissue. It should be used at least twice a week.
The effectiveness of Multi-Oral RemiDent was proven in an in vitro clinical trial aimed at comparing the hardness of normal enamel with the enamel eroded by a soft drink. The study also provided a comparison of the hardness of the enamel remineralised by Multi-Oral RemiDent and by artificial saliva.
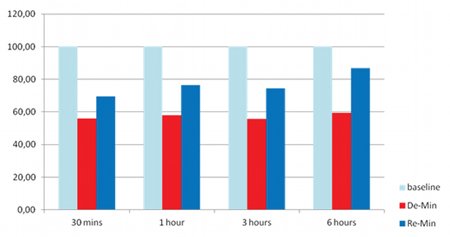
Figure 2: Experiment group with Multi-Oral RemiDent: results showing increased re-mineralisation with Multi-Oral RemiDent
After the teeth were demineralised with a soft drink, Multi-Oral RemiDent was applied to the surfaces of the teeth. After 30 minutes (min), 1 hour (hr), 3 hrs and 6 hrs the hardness of the enamel was measured again. Five human teeth were used for each measurement point.
Figure 1 shows the results of the control group with regular human saliva. It shows that the hardness of the tested tooth was decreased from 52.74% to 51.88% after 30 mins and after 6 hrs, the tooth hardness only increased from 48.60% to 51.03% with human saliva. Figure 2 shows that the hardness of the tested tooth increased from 55.83% to 69.5% 30 min after application of Multi-Oral RemiDent, and it even increased to 86.8% after 6 hrs.
Multi-Oral RemiDent increased the micro-hardness of the enamel that was eroded by a soft drink even more than artificial saliva did.
References
1. http://www.blackwellpublishing.com/trun/pdfs/Chapter12.pdf
2. McDonald RE, Avery DR, Stookey GK. Dental caries in the child and adolescents. DR, Dean JA, editor. Dentistry for the child and adolescent. 8th ed. New Delhi: Elsevier; 2005. p203-235.
3. Shafer WG, Hine MK and Levy BM. ED. A text book of oral pathology 5th Ed. Philadelphia WB Saunders company.1993; 567-658.
4. Ruhl S. Expert Rev Proteomics. 2012. 9(1). 85-96.
5. Lavelle LB Christopher Applied oral physiology, 2nd edition. Butterworths and Co (publishers) Ltd 1988. Saliva. p128-141.






