The body’s circadian rhythms – the normal variations in physiological parameters during the day – are very closely involved in regulation of sleep patterns. If these rhythms become out of synch, sleep patterns tend to be disrupted. Melatonin, a hormone produced in the pineal gland, is involved in the sleep–wake cycle of the circadian rhythm. It is excreted in response to a cascade of signals resulting from changes in light level, and the level that is present in the bloodstream varies through the day, with its release eventually resulting in the process of falling asleep.
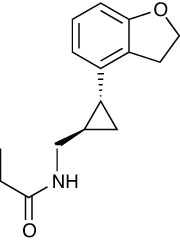
Melatonin can be used to treat sleep disorders, but it has poor bioavailability, and has a half-life in the body of only about 15 minutes. In addition, side-effects can be an issue as it binds non-selectively to many different receptors within the brain. As a result, there has been a degree of interest in analogues, and one, Takeda’s ramelteon (Rozerem) is approved in the US. Another, tasimelteon, is being developed by Vanda Pharmaceuticals, under licence from Bristol-Myers Squibb.1 It acts as a selective agonist at the MT1 and MT2 melatonin receptors in the brain’s suprachiasmic nucleus, which is a group of neurons in the anterior hypothalamus.
In a Phase II trial in induced insomnia, 39 healthy subjects were monitored for seven nights – three at baseline, three after a five-hour advance of the sleep-wake cycle with treatment with 10, 20, 50 or 100mg of tasimelteon or placebo before sleep, and a further night after treatment.2 The drug reduced sleep latency, and also increased sleep efficiency compared with placebo, with the shift in plasma melatonin rhythm being dose-dependent.
The same team also carried out a Phase III study in 411 healthy individuals who had transient insomnia induced in a sleep clinic by, again, a five-hour advance of the sleep–wake cycle. The subjects were given 20, 50 or 100mg doses or placebo 30 minutes before bedtime.2 Again, sleep latency and sleep efficiency were both improved, as was sleep maintenance. The adverse event patterns were similar for both treated and placebo groups.
It is also being investigated as a potential treatment for non-24 hour disorder, and it has orphan status in both the US and Europe. Patients with this rare disorder of the circadian rhythms are unable to synchronise their body clock within the 24-hour day-night cycle. Most totally blind people are affected as they do not have the sensitivity to light that is required to entrain the master body clock within the brain. Typically, the body clock runs longer than 24 hours, so people suffering from non-24 find it constantly delays and their circadian rhythms are regularly out of synch with night and day patterns.
In a Phase III study, 84 totally blind subjects were given 20mg daily doses of tasimelteon or placebo one hour before bedtime for three months.3 Nearly a quarter – 20 – of patients given the drug achieved a clinical response on the non-24 clinical response scale, and more than half had increased sleep in the worst quartile of nights.
The 20 who responded were randomised to continue treatment or receive placebo for two months, and those who continued on the drug maintained the entrainment of their circadian rhythm, while discontinuation led to loss of entrainment.4
References
1. N.N. Vachharajani et al. H. Pharm. Sci. 2003, 92, 760
2. S.M. Rajaratnam et al. Lancet 2009, 373, 482
3. S.W. Lockley et al. 27th Ann. Meet. Assoc. Prof. Sleep Socs (2013, Baltimore 3–5 Jun), LBA5
4. S.W. Lockley et al. ENDO (2013, San Francisco, 15–18 Jun), SUN-137






