Although it does occur in younger people, it is primarily a disease of the elderly. Five-year survival rates are low (24%) for those with intrahepatic disease. The primary treatment is surgery.
Later stage cancers cannot be entirely excised surgically. In these cases, radiotherapy and chemotherapy may be given, but there is no more specific drug treatment.
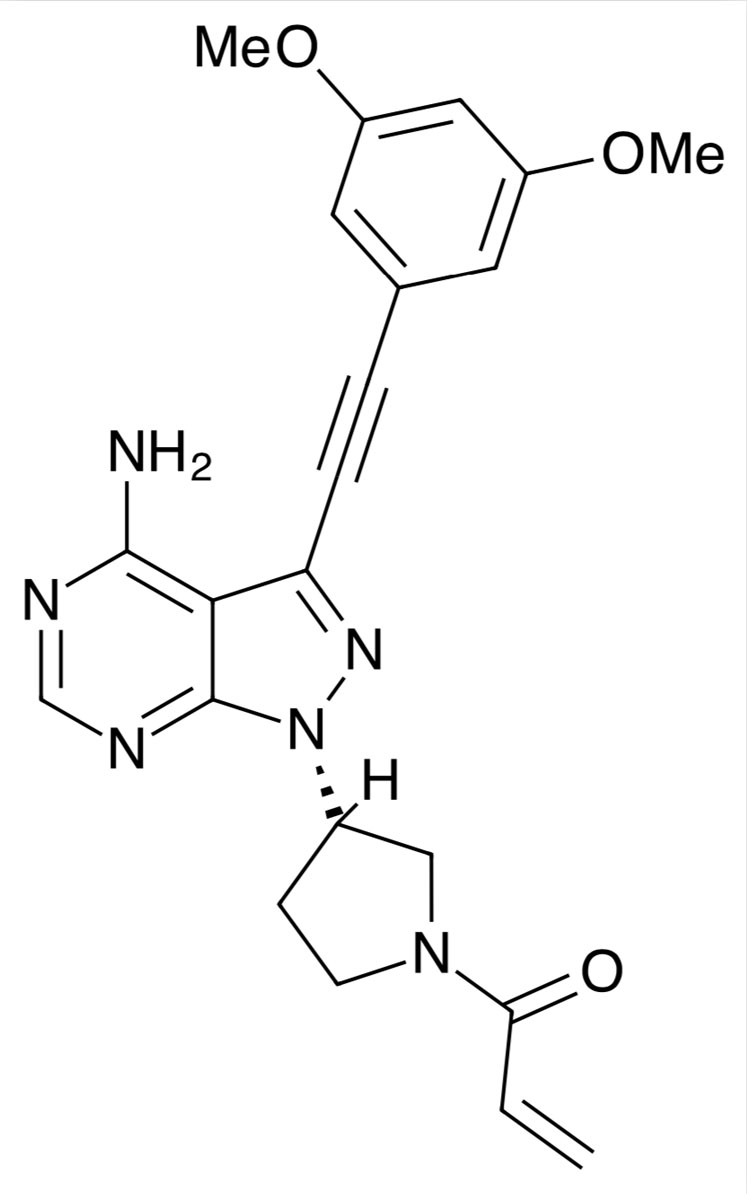
A new treatment is under development. Taiho’s futibatinib is an orally available selective, irreversible small molecule inhibitor of fibroblast growth factor receptors (FGFRs) 1, 2, 3 and 4, and is being developed as a potential treatment for patients with advanced solid tumours with genetic aberrations to FGFR 1–4, including cholangiocarcinoma.
The molecule binds to the FGFR binding pocket, inhibiting the signal transduction pathways it mediates, reducing tumour cell proliferation and increasing cell death in tumours with these mutations.
A first-in-human Phase I dose escalation trial has been done in 86 patients with advanced solid tumours that were refractory to standard therapies.1
Subjects were given 8–200 mg of the drug three times a week or 4–24 mg once a day. In all, 83% of the subjects had tumours with FGF/FGFR aberrations.
The maximum tolerated dose was determined to be 20 mg once a day, with no maximum tolerated dose defined for the thrice weekly schedule.
The most common treatment-emergent adverse events were hyperphosphataemia, diarrhoea and constipation, which led to dose interruptions and reductions or discontinuation in 55, 14 and 3% of patients, respectively.
Partial responses were seen in five patients, three of whom had FGFR2 fusion-positive intrahepatic cholangiocarcinoma (iCCA) and the other two had FGFR1-mutant primary brain tumours. Stable disease was achieved in a further 41 patients.
In a single-arm Phase II study, 103 patients with locally advanced or metastatic unresectable iCCA with FGFR2 gene fusions and disease progression after at least one line of systemic therapy were given daily 20 mg doses of the drug until disease progression or unacceptable toxicity occurred.2
In a preliminary analysis, data were reported for 67 patients with at least 6 months of follow-up, there was an objective response rate of 34.3%, a median time to response of 1.6 months and a median duration of response of 6.2 months.
Subgroup analysis of these interim data indicated that for those patients with confirmed FGFR2 alterations, the objective response rate was 36.2% for those with FGFR2 fusions and 44.4% for those with rearrangements.3
A further analysis showed that the 20 mg daily dose was encouraging in terms of patient-reported quality of life scores.4
References
- R. Bahleda, et al., Ann. Oncol. (2020): doi: 10.1016/j.annonc.2020.06.018.
- L. Goyal, et al., J. Clin. Oncol. 38(Suppl.), Abst. 108 (2020).
- J Bridgewater, et al., ESMO Virtual Congress 2020 (September 19–21), Abst. 4493.
- J.W. Valle, et al., ESMO Virtual Congress 2020 (September 19–21), Abst. 4513.






