Successful organ transplantation relies on immunosuppressant drugs to prevent organ rejection
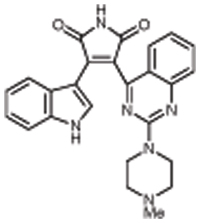
Successful organ transplantation relies on immunosuppressant drugs to prevent the body from rejecting the new organ. However, the available immunusuppressants such as cyclosporin and tacrolimus can have significant side-effects, including nephrotoxicity. Sotrastaurin is an alternative drug being developed by Novartis.1 It is a selective inhibitor of protein kinase C, which is involved in the activation of T cells, and thus blocks both early T cell activation and also the interleukin-2 production that follows.
Numerous early clinical trials have been carried out, including a randomised, three period crossover Phase I study in 18 healthy subjects looking at the combination effects of giving the drug in along with everolimus.2 Participants were given single oral doses of 100mg sotrastaurin, 2mg everolimus, and the combination of the two. The coadministration made no clinically relevant difference to the pharmacokinetics of sotrastaurin, and the area under the plasma drug concentration-time curve for everolimus was increased by 20% when given in combination with sotrastaurin.
Its effects in coadministration with tacrolimus were also investigated, with a similar trial design in 18 healthy subjects, with doses of 400mg sotrastaurin and 7mg tacrolimus.3 Tacrolimus had no effect on the pharmacokinetics of sotrastaurin, but again sotrastaurin had a positive effect on the AUC of the second agent, in this case doubling it. It appears to enhance the immunosuppressive activity of tacrolimus when given in combination.
A Phase II trial has also been carried out.4 A total of 216 patients undergoing kidney transplantation were given 200mg sotrastaurin twice a day in combination with either standard exposure or reduced exposure tacrolimus, or a control of standard exposure tacrolimus plus mycophenolic acid. In both sotrastaurin groups, patients were converted from tacrolimus to mycophenolic acid after the third month, achieving calcineurin inhibitor free immunosuppression. Composite efficacy failure rates were 5.4%, 1.5% and 4.1% respectively after three months, and 44.8%, 34.1% and 7.8% at the end of the study. These results led to a premature discontinuation of the trial. Leukopoenia and neutropoenia were more common preconversion in the control group. The initial combination with tacrolimus was efficacious and well tolerated, and the authors conclude that longer term evaluation of sotrastaurin plus tacrolimus is warranted.
References
1. J.P. Evenou J. Pharmacol. Exp. Ther. 2009, 330, 792
2. J.M. Kovarik et al. Int. J. Clin. Pharmacol. Ther. 2010, 48, 103
3. J. M. Kovarik et al. J. Clin. Pharmacol. 2010 Apr 12. [Epub ahead of print]
4. K. Budde et al. Am J Transplant. 2010 Jan 29. [Epub ahead of print]