Patients receiving a haematopoeietic stem cell transplant are also treated with an agent to...
Patients receiving a haematopoeietic stem cell - or bone marrow - transplant are also treated with an agent to mobilise the stem cells. This is typically granulocyte colony-stimulating factor (G-CSF) but there are large differences in response so new agents that have a more predictable effect would be extremely useful.
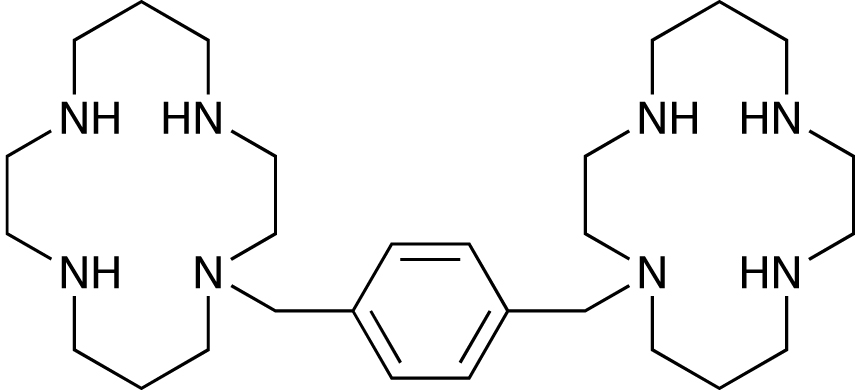
One such agent is Genzyme's plerixafor, acquired along with the company AnorMed.1 It acts at the CXCR-4 chemokine receptor, which has numerous signalling functions in the body, and also appears to be involved in stem cell mobilisation. The drug was originally designed as an anti-HIV agent, but was discontinued. However, it was also shown to increase peripheral leukocytes as it mobilised HSCs in the bone marrow by inhibiting the interaction between CXCR-4 and stromal cell-derived factor 1, and it is now being developed for this function.
In a Phase II study in autologous HSC transplantation in patients with relapsed or refractory Hodgkin lymphoma, 22 patients were given a combination of 10µg/kg G-CSF daily, plus 240µg/kg subcutaneous plerixafor 10-11 hours before apheresis.2 Results were compared with a historical control group who were given G-CSF alone. Two-thirds of the subjects met the primary endpoint of collecting at least 5x106 CD34+ cells/kg, and all bar one the minimum collection of 2 x106. This was a significant improvement over the historical control, and pharmacokinetics were similar to those seen in healthy volunteers.
Phase III trials have also been carried out. In one, 288 patients with non-Hodgkin's lymphoma undergoing autologous HSC transplantation were given 10µg/kg G-CSF for up to eight days, and then for four days from day four were also given 240µg/kg or placebo, with apheresis taking place daily from day five.3 The primary endpoint of 5x106 CD34+ cells/kg was met by 59% of those in the plerixafor group, and 20% of those given placebo.
As an add-on to this trial, patients on either arm who failed mobilisation were eligible for an open-label rescue protocol.4 These patients - 10 from the plerixafor arm and a further 52 from the placebo group - were given the same schedule again after a minimum seven-day rest period. Four of the pre-treated patients and 33 from the placebo group mobilised sufficient HSCs for transplantation. Common side-effects in the plerixafor group included mild gastro-intestinal effects and injection site reactions.
References
1. G. J. Bridger et al. J. Med. Chem. 1995, 38, 366
2. A. Cashen et al. Biol. Blood Marrow Transplant, 2008, 14, 1253
3. J. F. DiPersio et al. J. Clin. Oncol. 2009, 27, 4767
4. I. N. Micallef et al. Biol. Blood Marrow Transplant, 2009, 15, 1578