Blood clots may form, which can break loose and travel to the brain, causing an ischaemic stroke. The blockage caused by the clot prevents blood from reaching the brain and the resulting lack of oxygen causes brain cells to die.
If the patient survives, the long-term effects can include paralysis and a loss of speech or vision. Anticoagulant drugs are typically used to treat atrial fibrillation.
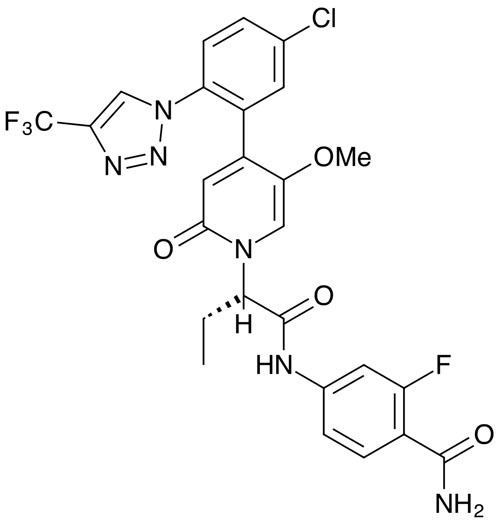
An alternative, the oral Factor XIa inhibitor asundexian, is being developed by Bayer.1
Factor XI is part of the blood coagulation cascade and is converted into its active enzyme form: Factor XIa (FXIa). This plays a critical role in the pathological formation of clots compared with normal clotting and uncouples haemostasis from thrombosis, leaving the pathway for clotting after injury intact.
Patients with a congenital deficiency in Factor XI have a lower risk of both venous thromboembolism and ischaemic stroke, but they rarely experience spontaneous bleeding. An inhibitor of FXIa could therefore act as an antithrombotic agent that still permits haemostatic clots to form in response to injury.
In a randomised, placebo-controlled, double-blind, parallel group Phase IIb dose finding study, 1808 patients were enrolled shortly after an acute non-cardioembolic ischaemic stroke.2
Subjects were randomised to receive 10, 20 or 50 mg daily oral doses of asundexian or a placebo, in addition to antiplatelet therapy. Treatment continued for a median of 70 days after randomisation and safety was comparable across all groups.
Although the trial was not powered to determine efficacy, at 26 weeks the primary efficacy outcome — dose-response effect on the composite of MRI-detected covert brain infarcts and recurrence of ischaemic stroke — was observed in 19% of both the placebo group and the 10 mg group, 22% in the 20 mg group and 20% of those given the highest doses.
In another double-blind, placebo-controlled Phase IIb trial, 1601 patients with a recent acute myocardial infarction (MI) were given 10, 20 or 50 mg of asundexian or a placebo for 6–12 months.3
Randomisation occurred within 5 days of the MI and they were also given dual antiplatelet therapy with aspirin and a P2Y12 inhibitor. The effect of asundexian on FXIa inhibition was assessed after 4 weeks and it gave a dose-related inhibition of FXIa activity; 50 mg doses gave greater than 90% inhibition.
There was no significant increase in bleeding and a low rate of ischaemic events. Again, the trial was insufficiently powered to assess efficacy. Phase III studies are now being planned to properly investigate its efficacy, with two trials expected to enrol 30,000 patients.
One will compare it with apixaban in atrial fibrillation and the other will look at its potential as an add-on to standard of care antiplatelet therapy to reduce the risk of ischaemic stroke in high risk patients.
References
- S. Heitmeier, et al., J. Thromb. Haemost. 20, 1400 (2022).
- A. Shoamanesh, et al., Lancet 400, 997 (2022).
- S.V. Rao, et al., Circulation 146, 1196 (2022).



