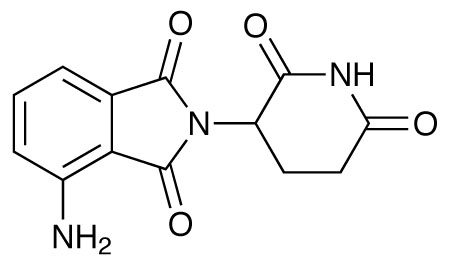
Thalidomide saw a renaissance when it was found to have potential to treat multiple myeloma because of its antiangiogenic activity – it inhibits TNF-alpha from monocytes. Analogues have been developed by Celgene to improve this inhibitory effect; pomalidomide, which has an additional amino group, is now being investigated not only in multiple myeloma but also in myelo-proliferative neoplasm associated myelofibrosis.1
In one trial, 60 patients with relapsed or refractory multiple myeloma were given 2mg oral doses of pomalidomide daily plus 40mg oral dexamethasone on days 1, 8, 15 and 22 of each 28-day cycle.2 Of these patients, 38 achieved a confirmed response, of which three had a complete response, 17 a very good partial response, and the remainder a partial response.
Responses were seen in 40% of those patients who were refractory to lenalidomide, 37% of those refractory to thalidomide, and 60% who were refractory to bortezomib. In addition, responses were seen in almost three-quarters of those with high-risk cytogenic or molecular markers. The majority of adverse events were related to myelosuppression, and the median progression-free survival time was 11.6 months.
Another trial compared pomalidomide plus low dose dexamethasone in patients whose myeloma was refractory with both bortezomib and lenalidomide.3 Two different dosing strategies were used – 2 or 4mg pomalidomide daily plus weekly 40mg doses of dexamethasone, with 35 patients in each cohort. In the lower group there were five very good partial responses, four partial responses and eight minor responses. In the other, there was one complete response, three very good partial responses, six partial responses and five minor responses. The overall survival at six months was 78% in the lower group, and 67% in the higher group; myelosuppression was again the most commonly observed toxicity.
It is also being investigated in myelofibrosis.4 A total of 94 patients took part in two consecutive clinical trials, in which they were given 0.5–3.5mg/day of pomalidomide, either with or without prednisone. The overall anaemia response was 27%, which increased to 53% for those patients positive for JAK2V617F with less than 10cm palpable splenomegaly and less than 5% circulating blasts; it was zero for mutation negative patients with greater splenomegaly and higher circulating blasts.
Trials continue; it is also being investigated as a potential add-on therapy to gemcitabine in patients with metastatic pancreatic cancer.5
References
1. G.W. Muller et al. Bioorg. Med. Chem. Let. 1999, 9, 1625
2. M.Q. Lacy et al. J. Clin. Oncol. 2009, 27, 5008
3. M.Q. Lacy et al. Blood 2011, 118, 2970
4. K.H. Begna et al. Am. J. Hematol. 2012, 87, 66
5. J.R. Infante et al. Eur. J. Cancer 2011, 47 199




