Guido Moosmann, of Schreiner MediPharm, argues that the current process of clinical trial supply management harbours inefficiencies that can be eliminated by innovative RFID-based technologies
When developing new drug-based therapies, the time to market is crucial. The total costs of developing a new drug or treatment up to its approval can amount to US$1bn (Euro 730m). Typically, a new drug has been subjected to about 10 years of stringent pre-clinical testing before entering the first of three clinical trial phases. Nonetheless, according to information published by the FDA in 2004, a new drug has just an 8% chance of achieving final approval and thus being brought to market.
One of the reasons for this is the fact that results obtained in animal tests can be applied to humans to only a limited extent. The vast majority (about 90%) of substances found to be "safe" with lab animals fail the test of subsequent clinical trials on humans.
Aside from the need to achieve high-quality test results, it is clear that the cost factors involved and the competitive environment require clinical trials to be run as expediently and smoothly as possible.
Often, the developer of a new drug will commission a contract research organisation (CRO) to perform the clinical trial. Whereas Phase I typically involves fewer than 100 people and lasts only for several weeks, Phase III may include as many as 10,000 people around the world and span several years. Like the drug inventors, the CROs, as service providers, are under immense quality and cost pressures during these studies.
Clinical Trial Supply (CTS) management is an essential element of clinical trials and, in addition to making and managing the trial samples, encompasses labelling and packaging functions, as well as the scheduled provision of the right IMPS (Investigational Medicinal Products) to investigation centres or investigators on an international scale.
In current best practice processes in CTS, materials and the associated information (see figure 1) are frequently separated. In addition, there is a considerable element of human influence on these processes, which can give rise to a high risk of errors. These potential errors are to be eliminated as much as possible by human controls. But the controls, by their nature, are also error-prone (figure. 2).
Hence processes are frequently controlled by the operator of the system, and not by the system itself. This may, for example, lead to quality-relevant data not being entered in the system in "real time" or, in extreme cases, not being entered at all.
Naturally, this is a potential source of errors, as a result of which the statutory control of the drug under test as well as the associated processes and information is no longer fully assured. errant practices
Currently, used processes do not automatically detect such errors. Consequently, if an error occurs, the process is not automatically stopped to correct it. Instead, the undetected error leads to consequential errors as the process continues. This "carry-forward" of errors may ultimately degrade the conclusive value and quality of the trial results in a major way.
In this scenario, errors are usually detected only if the trial drugs are not made available to the investigation centres or respective investigators as scheduled; or if deliveries have been made to the wrong site; or if someone has, in fact, identified any information as being incorrect or unavailable.
The example of a partial CTS management process, described below, serves to illustrate how "next practice" can eliminate the control issues and inefficiencies inherent in the current "best practice". The objective of this approach is to save time and costs as well as to contribute to a sustainable improvement of quality by eliminating potential sources of errors.
Essentially, this strategy automatically interlinks material and information flows and assigns the control functions to systems that allow human corrective intervention only in exceptional cases.
Labelling the drugs under test is one of the early steps in the process chain and offers an initial opportunity to achieve cost savings. As clinical trials are largely conducted on an international scale, the drugs have to be labelled with information in the languages of the respective countries.
As separate batches have to be produced for each country, this can be a complex and costly proposition, but special labels are available to remedy this problem. Depending on the requirements of the study, they can be designed as multilayered label versions or booklet labels providing enough space to accommodate all the language versions needed. In addition, detachable documentation labels, practical hanger functionalities, security features and RFID technology may be integrated into these solutions (see figure 3).
The labels serve to provide investigators, subjects and trial sponsors with information such as batch numbers, directions for use, the strength or potency of the drug, expiration date, package numbers, storage requirements and unique subject identifiers. Each clinical trial label identifies the packaged drug, the study and the subject participant with a unique identifier, such as a unique number, barcode or RFID tag, which ensures full traceability.
Figure 4 shows the optimised process of picking and packing a secondary packaging kit based on trial drugs marked with RFID technology in comparison with the process shown in figure 2.
This optimised process is based on marking each individual trial drug preparation with an RFID label, which may, for example, be invisibly embedded in a booklet label (figure 3). During the process of labelling the trial drugs the specific information is printed on the label. At the same time, the unique serial number is read by a printer-integrated RFID module and transmitted to the host IT system where it is "married" with the specific information on the label. If necessary, this specific data can be simultaneously programmed to the RFID chip and protected against tampering.
During the process of putting together the kits the system specifies the products to be included in the kit in the form of a "pick list". The finished kit is then automatically read at an RFID station, which is connected to the host IT system.
This means that the RFID labels of all the products contained in the kit are practically read simultaneously "through" the packaging and automatically compared with the pick list.
If the labels and the items on the list fully match, another RFID label is generated in the next process step. The operator applies this label to the kit after closing the kit. If necessary, this RFID label can be designed as a security label, providing irreversible evidence of the kit having been opened again after the operator has closed it and a visual indication of tampering with the package.
The unique serial number of the RFID label is linked by the system with the serial numbers of the RFID labels of the individual trial drug preparations inside the kit. This generates a hier-archical system, which automatically provides information about the contents when identifying the package.
Only when the contents of the kit and the pick list do not completely match (for instance, if the operator placed a wrong drug into the kit) will the system permit a corrective intervention by the operator. After the error has been corrected, the kit is subjected to a final, automatic reading process at the RFID station. If the contents of the kit and the items on the pick list fully match, the aforementioned RFID kit identification label is automatically generated and applied to the kit by the operator.
The controlling and checking functions that are currently performed by humans and, as such, are inevitably error-prone, will thus be delegated completely to a machine that works error-free. This means that any errors will be reliably detected by processes that are controlled by the system, then subsequently corrected by humans and, finally, checked again and automatically documented by the system.
Analogously, the subsequent processes of storage and shipping all the way to dispensing the drug to the patient or subject and the return of excess products can be RFID-based as well. In any event, such RFID-based solutions aim to transfer the control of processes from human operators to automated systems to eliminate time-consuming and costly error potential and to reduce a new drug's time to market.
There are further developments that can add significant value to clinical trial supply management. For example, in addition to just performing identification functions, RFID solutions with integrated sensors are able to document the temperatures to which the test drugs were exposed during storage and throughout the distribution chain up to the time of being dispensed to the subject.
This is of particular relevance as many clinical trials are conducted on an international scale, meaning test drugs have to be shipped across long distances and various climatic zones on their way from the manufacturer to the subject. Many new drugs, however, are temperature-sensitive and must therefore be stored, loaded, shipped and unloaded within a defined temperature window (e.g. 35.6-46.4°F or 2-8°C).
Otherwise the drug may lose its effectiveness or become totally unfit for use. In addition to air-conditioned means of transport, validated transport packaging, among other things, is used. This type of packaging has the capability of demonstrably maintaining the defined temperature conditions across specified time periods.
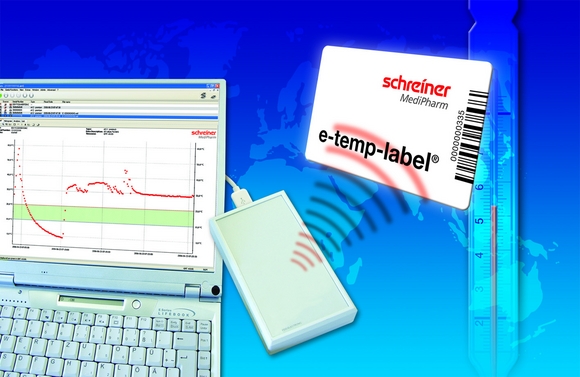
However, the "burden of proof" requires temperature conditions to be recorded and documented. For this purpose, temperature monitoring devices are used. The newest generation of such devices comes in the form of credit card-sized self-adhesive labels (figure 5).
These temperature monitoring labels are ideally suited for use in the range between -4° and -58°F (-20°C and 50°C). Thanks to an embedded, extremely flat battery they offer virtually unlimited service for a whole year. The labels are calibrated, have various operating modes, from short-term all the way to long-term monitoring periods, and are based on the international ISO 15693 RFID standard.
In addition, the labels allow flexible programming of the temperature range to be monitored and the temperature logging intervals. To a limited extent, even specific shipment information, such as a shipping ID code, may be written to the label.
Thanks to their small (credit card) size, such devices can even be accommodated in the smallest kits to document the temperatures inside the kit. With reference to the afore-mentioned RFID example, such a card can combine the purposes of the RFID identification label applied to the kit and the critical function of temperature monitoring.
In conjunction with qualified software tools that meet the requirements of use in a controlled environment (such as 21 CFR Part 11) the first solutions of this kind are now available as turnkey systems. In standard applications, they are operated as stand- alone systems but, if necessary, they may also be integrated into host IT infrastructures.
In summary, in many areas RFID technology has established itself and proven its viability as a means of optimising logistics processes.
However, effective use of RFID technology is based on the following two prerequisites:
1) recognition of the benefits that RFID can offer and
2) acceptance of the limitations that cannot (yet) be overcome by RFID.
There is no doubt that in the process of clinical trial supply management RFID can generate major value with regard to eliminating efficiencies and accelerating processes, thus also helping to make new, urgently needed drugs and therapies available to patients faster.






