This causes the overexpression of CSF1, leading to the recruitment of CSF1 receptor positive inflammatory cells into the lesion.
Dysregulation of this gene can cause TGCT inside or near to joints. Although benign, the tumours can grow and damage surrounding structures and tissues, leading to pain and swelling and limiting the movement of the joint.
It is commonly treated by surgery but the tumours tend to recur (particularly if diffuse). If surgery is not possible, treatment options are limited. A potential treatment, vimseltinib, has been developed by Deciphera, now part of Ono Pharmaceuticals.1
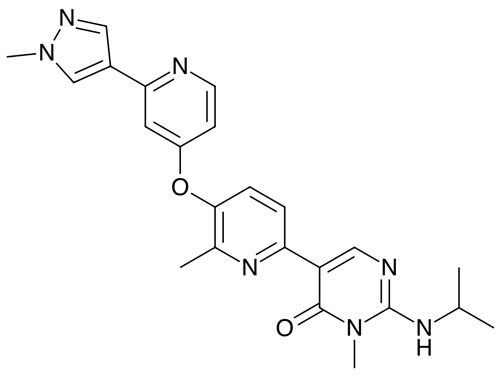
It is an oral switch control tyrosine kinase inhibitor that was designed to inhibit the CSF1 receptor (CSF1R).
In a first-in-human, open label Phase I/II study in 32 patients with TGCT who were not amenable to surgery or malignant solid tumours, the recommended Phase II dose was determined to be 30 mg twice a week (with no loading dose required).2
Most non-laboratory treatment-emergent adverse events had a severity of grade 1 or 2, with no evidence of cholestatic hepatotoxicity or drug-induced liver injury.
In TGCT patients, the median duration of treatment was 25 months with an objective response rate of 72%.
In a pivotal two-part randomised, double-blind, placebo-controlled Phase III study, 123 patients were recruited who had non-amenable-to-surgery TGCT and who had had no prior anti-CSF1 or anti-CSF1R therapy — although treatment with imatinib or nilotinib was permitted.3,4
In the first part of the trial, patients were randomised to receive either 30 mg of vimseltinib or a placebo twice a week for 24 weeks; in part two, those initially given the placebo had the option to receive vimseltinib, with all patients being able to receive the drug open label for the longer-term.
The primary endpoint, a statistically significant and clinically meaningful objective response rate by blinded independent radiological review, was seen at week 25. The rate was 40% with vimseltinib and 0% with the placebo.
Improvements in various secondary endpoints were also seen, including range of motion, whereby there was an 18.4% improvement from baseline with the drug versus 3.8% with the placebo.
Its safety profile was deemed to be manageable, with most non-lab treatment-emergent adverse events being grade 1 or 2. The company has recently submitted the drug for both EMA and FDA approval to treat TGCT patients.
References
- T.M. Caldwell, et al., Bioorg. Med. Chem. Lett. 74, 128928 (2022).
- H. Gelderblom, et al., Clin. Cancer Res. 30, 3996 (2024).
- W.D. Tap, et al., J. Clin. Oncol. 42(Suppl. 16), Abstr. 11500 (2024).
- H. Gelderblom, et al., Lancet 403, 2709 (2024).






